")
")
E. Titianova, I. Velcheva, B. Stamenov
Treatment of Acute Ischemic Stroke with Thrombolysis in Bulgaria
 Stroke is a socially significant disease characterized by high incidence, morbidity and mortality, causing severe disability worldwide. According to the World Health Organization there are 15 million new cases with stroke per year in the world; 5 million of them die and five million remain permanently disabled. In Europe, the annual stroke death is approximately 650,000 and mortality is higher in Central and Eastern Europe compared to Northern, Southern and Western Europe. In the European Union the total cost of cerebrovascular diseases amount 192 bilion euro annually; around 57% of them are health care costs, 21% are due to incapacity to work and 22% due to informal care of stroke survivals [9].
Stroke is a socially significant disease characterized by high incidence, morbidity and mortality, causing severe disability worldwide. According to the World Health Organization there are 15 million new cases with stroke per year in the world; 5 million of them die and five million remain permanently disabled. In Europe, the annual stroke death is approximately 650,000 and mortality is higher in Central and Eastern Europe compared to Northern, Southern and Western Europe. In the European Union the total cost of cerebrovascular diseases amount 192 bilion euro annually; around 57% of them are health care costs, 21% are due to incapacity to work and 22% due to informal care of stroke survivals [9].
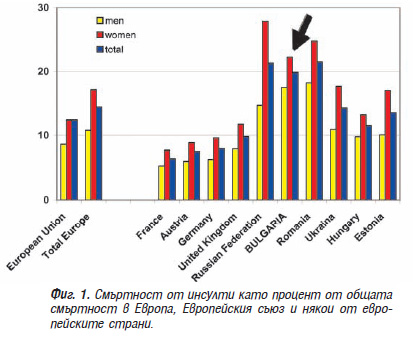
According to Eurostat data published in the EU information portal www.europa.eu, Bulgaria represents one of the most gloomy demographic pictures among the countries of the European Union. At the end of 2008, the country had the highest overall mortality (14.5 per 1000 population) and held a leading position in deaths from stroke – every fifth to sixth man and every fourth to fifth woman died from stroke, while in whole??? Europe deaths from stroke concern every tenth man and every seventh woman [9, 14]. Moreover, morbidity and mortality from stroke were significantly higher among the rural population [10, 13].
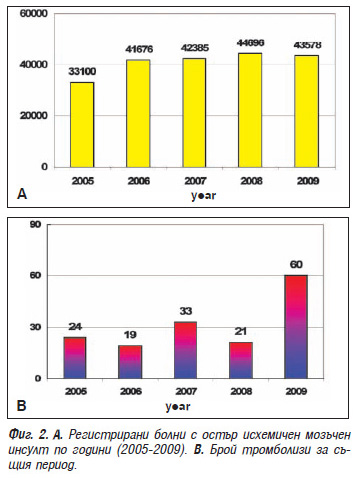
According to the Bulgarian Health Information Centre in 2009 50678 patients suffered from stroke and 95.8% (48,551) of them were hospitalized. The cases with acute ischemic stroke predominated – 85.6% (43,578 cases), 51.2% of them being women. The number of Bulgarians with stroke onset under 55 years of age was 4215 (9.7%). The men predominated – 5.6% as compared to women (4.1%), the latter having a greater mortality rate [8]. At the same time among the stroke sufferers disability reached 50-75%.
Analysis of the data from recent years shows three major trends in morbidity and mortality from stroke in Bulgaria: (1) as compared to 2004, the number of deaths from cerebrovascular disease in 2008 increased with 9.8% and mortality increased from 263.1 to 294.4/100 000 population (an increase with 31.3/100 000) (2). The number of women with ischemic stroke increases from 50.8% in 2006 to 51.2% in 2009 (3). The number of patients of both sexes who received ischemic stroke under the age of 55 decreases – from 11.9 % in 2006 to 9.7% in 2009. These trends are associated with the demographic process of aging of the Bulgarian population, where men have lower average life span [14] and with improved diagnostics of cardiovascular diseases and their endovascular treatment at younger age.
The thrombolytic therapy of acute ischemic stroke in Bulgaria with the application of recombinant tissue plasminogen activator (rt-PA) Actilyse® was introduced in 2005. The first thrombolysis was held in Plovdiv, Bulgaria [1]. The treatment is covered by the clinical pathway № 2 of the National Health Insurance Fund (NHIF) and it is performed in neurological clinic/ward with intensive care units with possibility for respiratory resuscitation according to the current medical standard "Neurological diseases" [5]. At the end of 2009 there are only 34 hospitals in Bulgaria, accredited for this treatment, which have contracts with the NHIF or about 10% of the hospital care establishments (mainly university, regional and some major municipal hospitals) and 27.6% from the multi-profile hospitals for active treatment. Moreover, only in one third of them venous thrombolyses have been realized – in Sofia, Varna, Plovdiv, Stara Zagora, Shoumen, Lom, Gabrovo Kyustendil (Fig. 2). Cases with thrombolytic therapy, unapproved by NHF because of failure of the clinical pathway protocol and possible cases in private hospitals without official information are not included in this statistics.
Analysis of the data by year shows that for the period 2005-2009 in the country 157 intravenous thrombolyses have been performed, which is substantially below the recommended minimum of 1-2% annually. Intra-arterial thrombolyses are significantly less frequent (below 10) and they are applied independently or in combination with endovascular recanalization only in Tokuda Hospital – Sofia [6].
 The absence of a national register for patients undergoing thrombolytic therapy does not allow to analyze the nationwide impact of therapy on the neurological deficit as assessed by NIHSS-scale. A significant regression of the neurological symptoms is reported only by Andonova S. [2] in 75% of the 20 patients treated by thrombolysis at University Hospital "St. Marina" – Varna. There is no accurate statistics for the complications of the treatment in the different centres. Our data show that they do not exceed 20%. So at the University Hospital in Varna 2 deaths (15%) due to the severity and location of stroke and only 1 haemorrhage (5%) as a complication of the treatment [2] were registered.
The absence of a national register for patients undergoing thrombolytic therapy does not allow to analyze the nationwide impact of therapy on the neurological deficit as assessed by NIHSS-scale. A significant regression of the neurological symptoms is reported only by Andonova S. [2] in 75% of the 20 patients treated by thrombolysis at University Hospital "St. Marina" – Varna. There is no accurate statistics for the complications of the treatment in the different centres. Our data show that they do not exceed 20%. So at the University Hospital in Varna 2 deaths (15%) due to the severity and location of stroke and only 1 haemorrhage (5%) as a complication of the treatment [2] were registered.
Regarding the rehabilitation of the patients after their discharge from the hospitals we did not find a reliable source of information. There is no official information about the degree of disability, the early and late survival rates after thrombolysis and the process of resocialization.
Compared to the countries in the European Community, the frequency of the thrombolytic treatment of acute ischemic stroke in Bulgaria is significantly below 1% – over the years it ranged from 0.04% (2006) to 0.1% per year (2009). Both worldwide and in Bulgaria, the main reason for the low frequency of this treatment is the late hospitalization of the patients – i.e. beyond the time when thrombolysis can be applied. Currently in Bulgaria it is applicable only in the first three hours after the onset of the ischemic stroke in persons from 18 to 75 years of age (for the European countries up to 80 years). Although the study ECASS III (European Cooperative Acute Stroke Study III) shows good safety and efficacy of the application of rt-PA between 3-4.5 hours from the beginning of symptoms [16], extending the therapeutic window for intravenous thrombolysis to 4.5 hours is not officially regulated in Bulgaria. This time interval may be increased to 4.5-6 hours when using intra-arterial thrombolysis and/or endovascular recanalization (mechanical extraction of the thrombus or stenting). However a number of contraindications exist, which makes the procedure inapplicable in many patients who reached the hospital on time. Other reasons for the limited use of intravenous thrombolysis in the treatment algorithm of acute ischemic stroke in Bulgaria are the lack of specialized units (stroke units) and qualified multi-disciplinary teams for implementation of the procedure; the limited number of hospitals with relevant equipment and human resources approved by NHIF, which do not cover the entire country territory; the absence of good correlation between the emergency teams and the hospital units performing the procedure; the lack of adequate information among the population, the emergency and outpatient departments about this therapy; the lack of a national register of stroke patients and a national program for stroke prevention. There exist financial restrictions for reimbursement of the treatment and organizational problems. Part of the problem is to be solved by the end of 2010 through updating the medical standard of Neurology, which regulates the creation of “stroke units” and the elaboration of a national health map, where their positioning will be regionalized.
The lack of sufficient information among the population for this kind of treatment is an important reason for the patients not to seek medical aid on time. Most often patients and their families do not know the symptoms of stroke and do not register the exact time of their onset. The media presentations of specialists are sporadic and are often associated with separate reports for successful thrombolyses and this is insufficient for the formation of an active public position on this topic.
The information among the medical specialists, particularly general practitioners, the outpatient and emergency teams is also insufficient. Scientific and practical information concerning the problem can be found predominantly in specialized neurological journals, distributed mainly among neurologists [3, 4, 5, 7, 15]. So far, the topic is poorly represented on scientific conferences. Recently an increased interest in thrombolysis for treatment of stroke has been observed, which is partly due to the implementation of endovascular recanalization methods [6, 11, 12].
Since 2009 the Bulgarian Association of Neurosonology and Cerebral Hemodynamics organizes various training activities for physicians to conduct thrombolytic therapy in acute ischemic stroke. The 4th Scientific Meeting of the Association held on October 3-4, 2009 in Hotel Rodina, Sofia with the participation of leading foreign specialists was devoted to thrombolysis [11, 12]. Workshops with the assistance of local hospital managers were organized in the towns of Gabrovo (2009) and Gotze Delchev (2010). Members of the Association took part in different activities of the Bulgarian Society of Neurology and in interdisciplinary symposia on endovascular therapy in carotid pathology, organized by the Association of Cardiologists in Bulgaria and the Bulgarian Society of Interventional Cardiology.
The President of the Association participated in the Round table for optimization of stroke treatment in Central and Eastern Europe, organized by Prof. Laszlo Csiba under the auspices of the European Stroke Organisation. The meeting was held on December 12, 2009 in Budapest. It ended with signing a statement from 17 representatives of 10 countries – Austria, Bulgaria, Poland, Romania, Russia, Serbia, Slovenia, Slovakia, Croatia and the Czech Republic, which is in press.
Analyzing these data by the end of 2009 it can be summarized that venous thrombolysis was not affirmed as a leading treatment of acute ischemic stroke in Bulgaria. Its frequency is significantly lower as compared to developed European countries and represents only 0.1% of the new stroke cases per year. Efforts are needed to adequate financing of the health care facilities, professional training of human resourses and education of the population by creating an unified national strategy as a state health policy. In this strategy optimal use of public-private partnership is strongly recommended.
In the present volume of the journal in a series of articles we summarize the experience in thrombolytic therapy of acute ischemic stroke in Bulgaria.

Книгопис
1. Андонова В, Мильотов И, Чаушева П, Георгиева Р, Молев А. Първи случай в България на тромболиза в острата фаза на исхемичния мозъчен инсулт. В: Девети национален конгрес по неврология с международно участие, 8-10 септември 2005. Българска неврология 5, 2005:200 (Р122).
2. Андонова С. Приложение на ултразвуковите методи при остър исхемичен мозъчен инсулт с тромболиза. В: Четвърта среща на Българската асоциация по невросонография и мозъчна хемодинамика с международно участие, 3-4 октомври 2009, София. Невросонография и мозъчна хемодинамика 5, 2009:123.
3. Велчева И. Тромболично лечение. В: Хаджиев Д, Лехнер Х (ред) Исхемичен инсулт. Арсо, 2001, 130–137.
4. Клисурски М. Сонотромболиза. Невросонография и мозъчна хемодинамика 2, 2006:61-66.
5. Медицински стандарт “Нервни болести”. Наредба №19/2.08.2006 на Министерство на здравеопазването. Държавен вестник бр.67/18.08.2006 г.
6. Петров И. Супраселективна фибринолиза и стентиране на интракраниални артерии при исхемичен мозъчен инсулт – пилотен опит. В: Четвърта среща на Българската асоциация по невросонография и мозъчна хемодинамика с международно участие, 3-4 октомври 2009, София. Невросонография и мозъчна хемодинамика 5, 2009:123.
7. Протокол за интравенозна тромболитична терапия при остро настъпили исхемични мозъчни инсулти (ИМИ) с Alteplase (Actilyse). Българска неврология 4, 2004:48-52.
8. Случаи на остра мозъчносъдова болест по диагнози за 2009 г. В: Оперативна информация. Национален център по здравна информация, София (www.nchi.government.bg)
9. Allender S, Scarborough P, Peto V, Rayner M, Leal J, Luengo-Fernandez R, Gray A. European cardiovascular disease statistics 2008 edition. Department of Public Health, University of Oxford, 2008. European Heart Network.
10. Georgieva L, Powles J, Genchev G, Salchev P, Poptodorov G. Bulgarian population in transitional period. Public Health and Peace 43, 2002:240-244.
11. Klein GE. Intraarterial thrombolysis and endovascular recanalization procedures in acute stroke. In: Fourth meeting of the Bulgarian Society of Neurososnology and Cerebral Hemodynamics with international participation, 3-4 October 2009, Sofia. Neurosonology and Cerebral Hemodynamics 5, 2009:122.
12. Niederkorn K. Intravenous thrombolysis in acute stroke – scientific evidence and practical aspects. In: Fourth meeting of the Bulgarian Society of Neurososnology and Cerebral Hemodynamics with international participation, 3-4 October 2009, Sofia. Neurosonology and Cerebral Hemodynamics 5, 2009:122.
13. Powles J, Kirov P, Feschieva N, Stanoev M, Atanasova V. Stroke in urban and rural populations in north-east Bulgaria: incidence and case fatality findings from a 'hot pursuit' study. BMC Public Health, 2002; 2:24.
14. Public health statistics, Bulgaria 2009, Annual. National Center of Health Information. Sofia, 2009.
15. Ritter MA, Ringelstein EB. Neurososnology in acute stroke: a fascinating tool for diagnosis and treatment. Neurosonology and Cerebral Hemodynamics 1, 2005:5-9.
16. Schellinger P, Hacke W, Fiebach J. Thrombolysis with Alteplase 3 to 4.5 hours after acute stroke. (ECASSIII) N Engl J Med 359, 2008:2839-2841.